Pediatric Eyewear Dispensing: The Lens Material, Coating, and Frame Decisions That Actually Hold Up

Why Kids Aren’t Just Small Adults at the Dispensing Table
A pediatric patient changes four variables an adult dispense rarely has to account for at the same time.
Prescriptions shift faster. Axial growth and developing refractive error mean many pediatric patients are due for a new Rx well before eighteen months — sometimes annually, sometimes faster in progressing myopia. A lens decision made for “how this prescription behaves” has a shorter shelf life than it does for a 45-year-old presbyope.
Compliance is involuntary. An adult who finds a coating uncomfortable simply stops wearing the glasses and tells you why at the next visit. A child does the same thing without the explanation – the glasses end up in a backpack, a desk drawer, or nowhere, and the practice finds out at the next exam when the prescription has gone uncorrected for months.
Physical handling is aggressive by default. Sports, falls, siblings, being sat on, being used as a slingshot, being left lens-down on asphalt – none of this is misuse from a child’s perspective. It’s just what a school day looks like.
And self-report is unreliable. A child experiencing glare, a poor optical center, or a frame pressing on the temple often can’t isolate the cause. The parent reports general frustration: “He keeps taking them off.” Diagnosing why falls entirely on the original dispensing decisions, because the patient can’t help you triage it.
Material, coating, and fit choices that would be reasonable defaults for an adult can quietly fail a pediatric patient on all four of these variables at once.
Lens Material: Where the Decision Mostly Makes Itself
Every prescription lens sold in the U.S. has to clear a baseline impact-resistance standard. For pediatric and active patients, baseline isn’t the target.
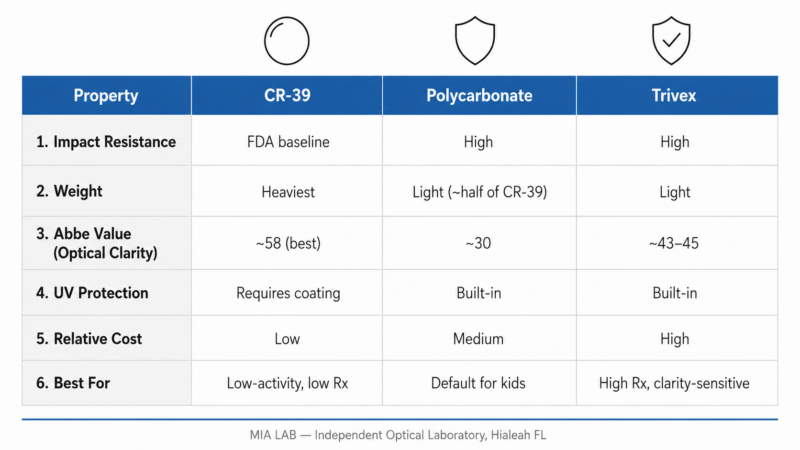
The American Academy of Ophthalmology and most pediatric optometric guidance point in the same direction: polycarbonate lenses or Trivex as the default for children, full stop, with CR-39 reserved for specific cases where a parent has explicitly weighed the trade-offs.
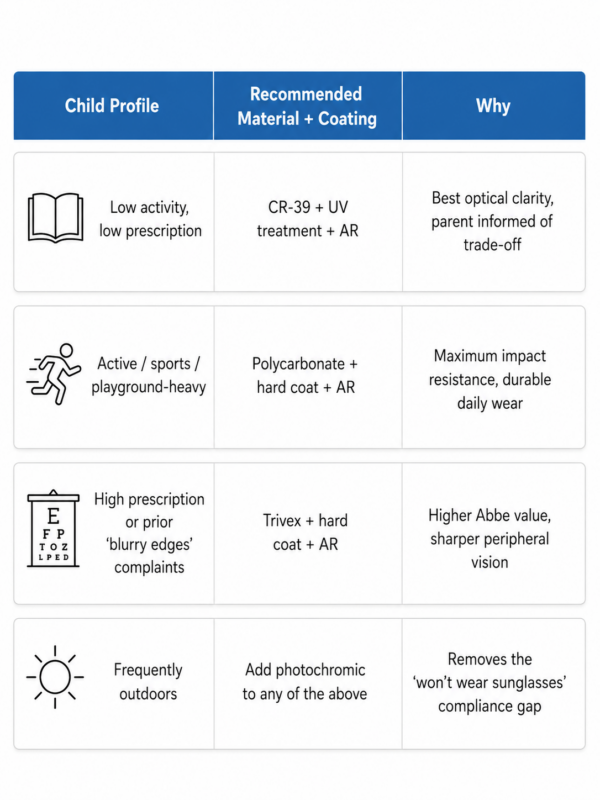
Polycarbonate lenses are the long-standing default for a reason. They’re significantly more impact-resistant than standard plastic, roughly half the weight of CR-39 in comparable prescriptions, and carry built-in UV protection without an added treatment. The trade-off is optical: a lower Abbe value means more chromatic aberration at the lens periphery, which is rarely something a child will articulate but can show up as “things look weird at the edges” if you ask the right question.
Trivex narrows that trade-off. Impact resistance is comparable to polycarbonate lenses, weight is similar or slightly lower, and the Abbe value is meaningfully higher – closer to CR-39’s optical clarity. For a higher prescription or a child who has previously complained about “blurry edges” in polycarbonate lenses, Trivex is worth the conversation even at a higher material cost.
CR-39 still has a place – a low-prescription, low-activity child whose parent prioritizes optical clarity and is fully informed about the impact-resistance gap. It should never be the unexamined default for a pediatric patient simply because it’s the practice’s standard plastic.
This is the same material logic covered in detail in our broader lens material comparison, but the pediatric stakes raise the cost of getting it wrong: a CR-39 lens that shatters on contact isn’t a remake conversation. It’s a different kind of conversation entirely.
Coatings That Survive an Actual Childhood
Coating decisions for kids should be evaluated against one question that doesn’t come up as often in adult dispensing: how does this perform after six months of being handled with whatever was on the child’s hands at the time?
Scratch resistance isn’t optional
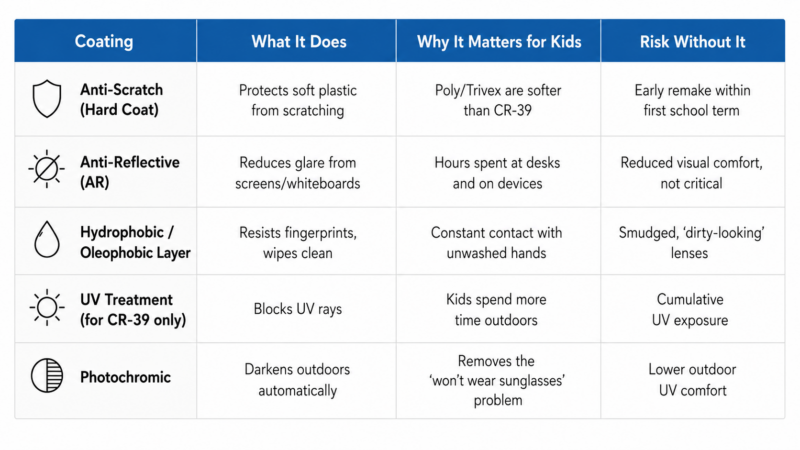
Polycarbonate and Trivex are both softer than CR-39 and need a quality hard coat to perform acceptably. Skipping or underspeccing this coating on a pediatric lens isn’t a cost saving – it’s a guaranteed remake within the first school term.
Anti-reflective coating: still worth it, with one caveat
AR coating reduces glare for the hours kids spend looking at screens and whiteboards, and it remains clinically worth recommending – see our comparison of premium AR coatings for how the major coating tiers differ. The caveat is durability: a budget AR coat on a lens that gets touched constantly by small, often unwashed hands will show smudging and degradation faster than the same coating on an adult’s glasses. A hydrophobic, oleophobic top layer that resists fingerprints and wipes clean without streaking matters more here than on almost any other patient category – and it’s worth walking parents through proper cleaning technique at dispense, since most lens damage attributed to “bad coating” is actually dry-wiping with a shirt hem.
UV protection: built in, not optional
Children spend disproportionately more time outdoors relative to their lifetime sun exposure than adults do. Polycarbonate lenses and Trivex carry UV protection inherently; if a practice dispenses CR-39 for a pediatric patient, a UV treatment isn’t a suggested add-on, it’s a requirement.
Photochromic: a genuine convenience, evaluated honestly
For an active, frequently-outdoors child, a photochromic lens removes the friction of swapping to sunglasses – friction that, per the compliance problem above, usually means the sunglasses just don’t get worn. The honest caveat to give parents: photochromic lenses won’t darken meaningfully behind most car windshields, so the convenience is for recess and the playground, not the carpool line.
Frame Fit and PD: The Measurement Problem Unique to Pediatric Dispensing
Pupillary distance measurement on a cooperative adult is routine. On a squirming four-year-old, it’s a different skill – and the cost of getting it wrong is higher than it is for an adult, because a child is far less likely to report the headaches, eye strain, or “things look weird” symptoms that come from a poorly centered optical zone. They just stop wearing the glasses, and the practice never learns why.
Frame selection compounds the problem. A frame that fits perfectly at dispense may not fit in four months – growing faces change temple length and bridge fit faster than most parents think to mention. Spring hinges that tolerate repeated, careless removal, temples with enough adjustability to track growth between exams, and a bridge fit that doesn’t rely on a static measurement all reduce the number of “these don’t fit right anymore” visits that otherwise get mistaken for lens complaints.
None of this is solved by ordering a smaller version of an adult frame and lens combination. It’s solved by treating pediatric measurement and frame fit as their own clinical step, not an abbreviated version of the adult workflow.
What This Means for Your Practice — and Your Lab Relationship
Pediatric remakes carry a different cost structure than adult remakes. Most aren’t lab errors – they’re breakage, loss, or growth. But the practice still absorbs the relationship cost: a parent who has been back three times in a school year forms an opinion about your practice’s reliability, even when every individual remake was reasonable.
Two things change that dynamic. The first is the backup pair conversation – the same second-pair logic that applies to occupational lenses applies differently here: a low-cost backup pair in polycarbonate lenses, dispensed at the same visit as the primary pair, turns an inevitable breakage event from an emergency into a non-event. Practices that build this into the pediatric dispensing sequence consistently report fewer panicked same-week calls.
The second is turnaround. A child without correction doesn’t just lose comfort – they lose access to the blackboard and the page in front of them, which makes pediatric remakes a different kind of urgent than an adult’s. A lab partner that ccan turn a single-vision remake in polycarbonate lenses around quickly, with quality control tight enough that the replacement doesn’t introduce a new problem, removes a meaningful piece of stress from a conversation parents are already having with some guilt attached.
This is where an independent optical lab that finishes polycarbonate lenses and Trivex lenses in-house earns its place in the pediatric workflow specifically. At MIA LAB, in-house finishing and a 24-hour turnaround on uncut lenses mean a broken pediatric pair doesn’t sit in a queue behind everything else, and bilingual support means the material and coating trade-offs above can be explained to a parent in whichever language makes the decision actually land.
The Decision That’s Actually Being Made
A child’s glasses aren’t a fashion accessory and they aren’t a smaller version of an adult prescription. They’re the only access that child has to a clear blackboard, a clear soccer ball, a clear face across the dinner table, for every waking hour of the day.
The material, coating, and fit decisions made at the first dispense are the difference between glasses that survive a school year and glasses that come back in week three.
Get them right once, and most of what looks like a behavior problem on a Tuesday afternoon turns out to have been a dispensing decision all along.
FAQ: Lens Materials and Coatings for Pediatric Dispensing
- What is the best lens material for children’s glasses?
Polycarbonate lenses or Trivex, in nearly all cases.. Both clear a significantly higher impact-resistance bar than standard CR-39 plastic, both are lighter, and both carry built-in UV protection. CR-39 should only be considered for a low-activity child whose parent has been informed of the trade-off and still prefers the optical clarity.
- Is Trivex or polycarbonate better for kids?
Impact resistance is comparable between the two. Trivex offers a meaningfully higher Abbe value, which translates to less chromatic aberration and sharper peripheral vision, particularly relevant for higher prescriptions. Polycarbonate lenses are typically the lower-cost default; Trivex is worth recommending when optical clarity complaints have come up before or the prescription is higher.
- Do kids’ lenses need anti-reflective coating?
Yes, for the same reasons adults benefit from it, plus the practical reality of screen time and classroom lighting. The decision that matters more for pediatric patients is coating durability – a hydrophobic, oleophobic top layer that resists smudging from frequent handling will outperform a basic AR coat over the life of the glasses.
- Are scratch-resistant coatings really necessary for pediatric lenses?
Necessary, not optional. Polycarbonate and Trivex are softer materials than CR-39, and a pediatric patient’s daily handling all but guarantees early scratching without a quality hard coat. Underspeccing this coating to save cost on a pediatric order is one of the more reliable ways to generate an early remake.
- Should children get photochromic lenses?
For an active, frequently-outdoors child, yes – photochromic lenses remove the compliance problem of swapping to separate sunglasses, which often just don’t get worn. Set the expectation with parents that photochromic lenses won’t darken significantly behind most car windshields, so the benefit applies to outdoor time, not car rides.
- How do you get an accurate PD measurement on a young or uncooperative child?
Take the measurement at the moment the child is calmest and most distracted, ideally with a second set of hands, and verify with a second method (pupillometer plus a manual cross-check) rather than relying on a single reading. A poorly centered optical zone is one of the most common, least diagnosed causes of a child quietly refusing to wear new glasses.
- How often should a child’s glasses be reassessed for fit?
More often than the prescription itself. Facial growth, especially in younger children, can outpace the annual exam cycle. A quick fit check at any sick visit, sports physical, or convenient touchpoint catches temple and bridge issues before they turn into a lost-and-broken-glasses cycle.
- What should a practice do when a child’s glasses break shortly after dispensing?
Diagnose before reordering. If it’s the second or third break in a short window, the issue is more likely the original material, coating, or fit decision than the child’s behavior. Pair this with a fast-turnaround lab relationship and, where appropriate, a low-cost backup pair conversation at the next visit to reduce the chance of a repeat emergency.


