How Progressive Lenses Work: A Practical Guide for Optical Practices

Progressive lenses are one of the most recommended and most misunderstood products in optical. In clinical practice, these patterns repeat consistently and they are rarely caused by the lens alone.
Patients hear “no-line multifocal” and expect seamless vision. Sometimes they get it.
Sometimes they say: “Something feels off.”, “I can’t find the right spot.” or “My old lenses felt easier.”
That gap between expectation and experience is not random. It is the result of how progressive lenses are designed, how they are fitted, and how consistently they are manufactured.
This guide explains how progressive lenses work, how lens design and digital freeform technology affect vision, and what determines whether they succeed or fail in real practice.
To understand how progressive lenses work in real practice, it’s important to look beyond the concept and focus on how patients actually experience them.
What Are Progressive Lenses? (And Why Patients Choose Them)
Progressive lenses are multifocal lenses that provide continuous vision correction across multiple distances without visible segment lines.
They are most commonly prescribed for presbyopia – when patients begin to lose near vision while maintaining distance clarity. Instead of switching between multiple pairs of glasses or relying on segmented lenses, progressive lenses allow a smooth transition between viewing distances within a single lens.
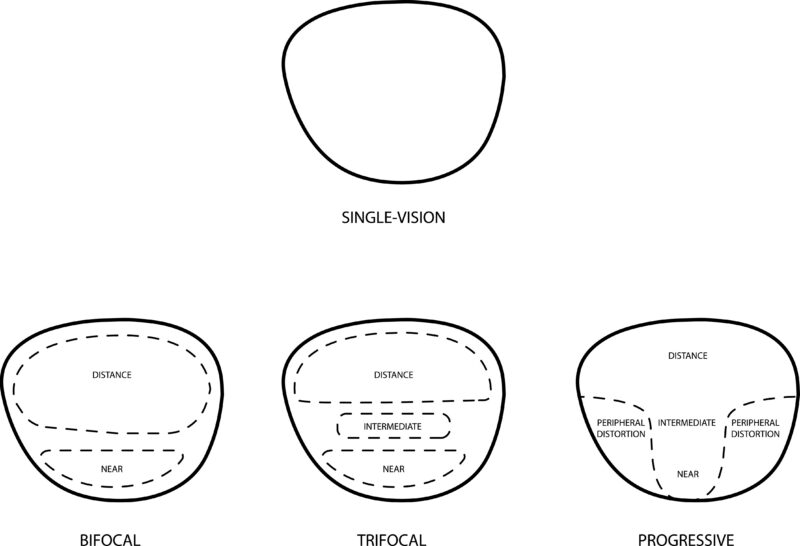
Unlike bifocals, which divide vision into two distinct zones, progressive lenses create a continuous gradient of power. That difference is not just cosmetic. It fundamentally changes how patients experience vision throughout the day.
For a deeper comparison between lens types, see:
https://mialab.com/blog/digital-progressive-lenses-vs-bifocals
How Progressive Lenses Work: The Optical Design Explained
At a glance, progressive lenses look simple. In practice, they are one of the most complex designs in ophthalmic optics.
Every progressive lens is built around a controlled distribution of power across its surface. The lens transitions from distance correction at the top to near correction at the bottom through a narrow vertical region known as the corridor.
The upper portion of the lens is designed for distance vision, the central corridor supports intermediate tasks such as computer use, and the lower portion provides near vision for reading and close work.
Patients do not consciously “switch zones.” Instead, they adjust head and eye position naturally or struggle if the design does not align with their behavior.
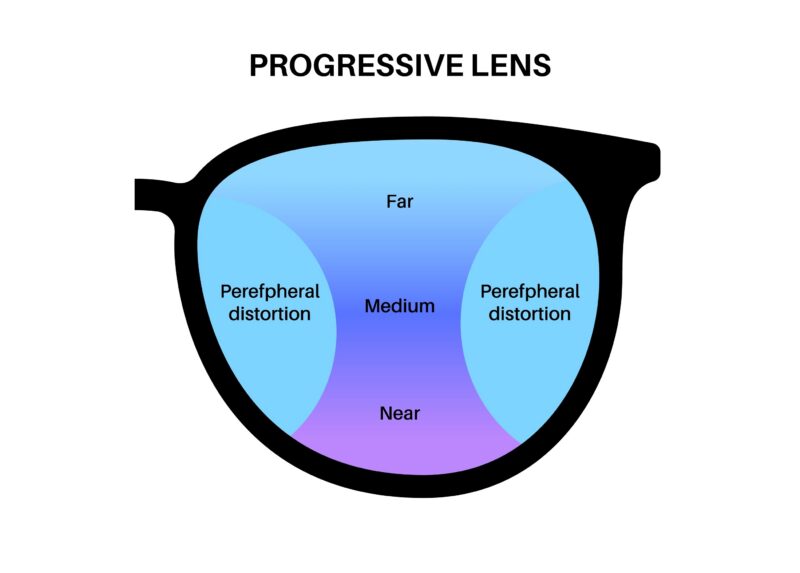
Why progressive lenses create both clarity and distortion
To achieve a smooth transition between focal distances, lens designers must redistribute unwanted optical error. This error is pushed into the periphery, creating areas of distortion.
Patients experience this in simple terms: edges may feel less stable, head movement becomes more important, and overall visual comfort depends heavily on alignment.
This is not a flaw. It is a necessary compromise in progressive lens design.
How Digital Freeform Technology Improves Progressive Lenses
Traditional progressive lenses are based on standardized templates. Modern lenses are not.
Digital freeform surfacing allows the lens surface to be calculated and manufactured point-by-point at a micron-level precision
Learn more here:
https://mialab.com/what-is-freeform-technology-in-optical-lenses
With digital surfacing, the lens becomes more responsive to real-world use. Distortion can be redistributed more effectively, corridor design can be optimized, and visual transitions become more stable.
The result is not just better optics on paper – it is a noticeable difference in how quickly patients adapt and how confident they feel wearing the lenses.
Why Personalization Matters More Than Technology Alone
Even the most advanced progressive lens design fails when it is applied without context.
In theory, digital freeform technology allows for extremely precise lens surfaces. In practice, that precision only matters if it is aligned with how the patient actually wears and uses their glasses. A progressive lens does not exist in isolation – it exists on a face, in motion, under real conditions.
A frame that sits slightly lower changes the position of the corridor. A patient who works eight hours at a desktop will use the intermediate zone far more than someone who primarily drives. A person who reads in bed will approach near vision from a completely different angle than someone reading at a desk.
When these factors are not accounted for, the lens may still be technically correct – but it will not feel natural.
Patients rarely describe this as a technical issue. Instead, they say things like: “I have to move my head too much,” or “It’s clear, but it doesn’t feel right.” What they are experiencing is a mismatch between lens geometry and behavior.
This is where personalization becomes decisive. Not as a premium feature, but as a functional requirement.
In a well-executed process, the lens design is selected based on how the patient actually lives: how they hold their head, how they move their eyes, how they divide time between near, intermediate, and distance tasks. Frame parameters are measured accurately, not estimated. The goal is to align the usable zones of the lens with the patient’s natural posture, not force the patient to adapt to the lens.
From the patient’s side, the most important takeaway is simple: if vision feels slightly “off,” it is often not a limitation of progressive lenses as a category. It is a sign that the lens has not been fully aligned with how they use their vision. When that alignment is corrected, the difference is immediate – not subtle.
Personalization is what turns progressive lenses from something patients tolerate into something they stop thinking about entirely.
Why Some Progressive Lenses Feel “Hard to Adapt”
When patients struggle with progressive lenses, the issue is rarely random – and almost never imaginary.
What makes progressive lenses unique is also what makes them sensitive. They require coordination between lens design, frame position, eye movement, and patient behavior. When one of these elements is even slightly misaligned, the lens still works – but it no longer feels intuitive.
Patients describe this in very specific ways. They may feel slightly unsteady when walking, even though their vision is technically sharp. They may notice that reading is clear, but transitioning to a screen requires effort. They may find themselves searching for the right angle instead of naturally finding it.
From a clinical perspective, these are not vague complaints. They are highly accurate signals.
In most cases, what the patient is experiencing is not poor vision, but increased cognitive load. The visual system is working harder than it should to maintain clarity. Instead of vision being automatic, it becomes something the patient has to manage.
This usually traces back to one of three underlying issues: the corridor is not aligned with natural gaze patterns, the frame position shifts the effective zones of the lens, or the optical quality of the lens (including material and coating) introduces subtle instability that becomes noticeable over time.
The key point is that these factors do not operate independently. They compound. A slightly low fitting height combined with a narrow corridor and a glare-prone coating does not create three small problems – it creates one noticeable experience of discomfort.
What matters in practice is how this is handled.
Dismissing adaptation concerns or asking patients to “give it more time” often makes the situation worse. A better approach is to treat the complaint as useful data. When discomfort appears during walking, it points toward peripheral distortion or frame alignment. When it appears at a computer, it often indicates corridor placement or design mismatch. When the complaint is fatigue rather than blur, material or coating may be contributing.
In many cases, the solution is not a full remake, but a targeted correction: adjusting the frame, refining measurements, or selecting a design that better matches the patient’s actual visual behavior.
The most important insight is this: when a patient says “something feels off,” they are usually describing a real mismatch within the system. Progressive lenses do not fail silently. They communicate through perception. The role of the practice is to interpret that signal correctly – and respond with precision.
Related reading:
https://mialab.com/lens-material-guide-choosing-the-best-lens-material-for-every-prescription
https://mialab.com/anti-reflective-coating
Types of Progressive Lenses Explained
Not all progressive lenses are designed for the same purpose, even if they share the same basic structure.
Standard progressive lenses rely on pre-set designs, which makes them easier to produce but less adaptable. Digital progressive lenses improve precision by adjusting the surface to the prescription and frame. Occupational lenses shift focus toward intermediate and near vision, making them more suitable for desk work and screen use. Custom progressive lenses go further, aligning design with individual parameters to improve comfort and reduce adaptation time.
Understanding these differences allows practices to move from “selling lenses” to recommending solutions.
Progressive Lenses vs Bifocals: Key Differences
Bifocals divide vision. Progressive lenses connect it.
The difference is not only visual but behavioral. Progressive lenses allow continuous vision without visible lines, which improves aesthetics and provides a more natural viewing experience. Bifocals remain relevant in specific cases but are increasingly replaced by progressive designs in modern practice.
For a detailed comparison:
https://mialab.com/blog/digital-progressive-lenses-vs-bifocals

How to Improve Patient Adaptation to Progressive Lenses
Successful adaptation is not a coincidence. It is the result of a controlled process inside the practice.
Adaptation success depends on three elements working together: accurate measurements and frame fitting, clear communication about what to expect, and proper alignment between lens design and the patient’s lifestyle.
When these elements are consistent, adaptation improves dramatically and remakes decrease.
How an Optical Lab Influences Progressive Lens Performance
The final performance of a progressive lens is not defined only by design. It is defined by execution.
Even a well-designed lens can fail if manufacturing lacks precision or consistency.
Why manufacturing quality matters
Progressive lenses are highly sensitive to surfacing accuracy. Small deviations affect corridor placement, clarity, and overall comfort.
Consistency is what reduces remakes
Reliable production ensures that lens geometry remains consistent, coatings perform as expected, and turnaround times stay predictable.
This reduces variability – and variability is the main driver of remakes and patient dissatisfaction.
For independent practices, the difference between average and premium results often comes down to lab quality.
If you’re evaluating options, start here:
https://mialab.com/how-to-choose-the-best-optical-lab
A strong optical lab partner does not just supply lenses. It stabilizes outcomes.
FAQ: Progressive Lenses Explained
How long does it take to adjust to progressive lenses?
Most patients adapt within several days to two weeks. Longer adaptation often indicates fitting or design mismatch.
Do progressive lenses cause distortion?
Yes, in the periphery. This is part of the design. The goal is to control and minimize its impact.
Are digital progressive lenses worth it?
In most cases, yes. They improve stability, reduce adaptation time, and provide a more predictable visual experience.
Why do patients say “something feels off”?
This typically reflects a mismatch between lens design, fitting accuracy, and patient expectations rather than a defect.
Final Perspective
Progressive lenses are not a single product. They are a system where design, fitting, and manufacturing must work in alignment.
Design, material, coating, fitting, and manufacturing must work together. When they do, patients stop thinking about their lenses.
In modern optical practice, that is the clearest indicator that the system is working as intended.


