IOT Digital Ray-Path Lenses: A Clinical Explanation for Optometrists

There is a difference between a lens that corrects a prescription and a lens that corrects how a specific person, wearing a specific frame, uses their vision throughout a real day. That difference has a name: IOT Digital Ray-Path technology. Understanding it — clinically, not just commercially — changes how you fit, recommend, and explain lenses to patients who need more than a standard solution.
What IOT Digital Ray-Path Actually Does
IOT stands for Indizen Optical Technologies, a Spanish optics company founded in 2002. Their Digital Ray-Path algorithm is the computational engine behind one of the most precise lens personalization systems in ophthalmic optics.
The core principle is ray tracing through a real optical system — not an idealized one.
Traditional progressive lens design calculates surface geometry based on an average wearing model. A standard pantoscopic tilt, a standard vertex distance, a standard frame position. These averages are reasonable for most patients but accurate for few of them. The discrepancy between the design assumption and the actual wearing position introduces optical aberrations that the patient experiences as blur, swim, or distortion at the periphery.
IOT Digital Ray-Path 2 — the current generation — eliminates this assumption. Instead of calculating lens performance as if the patient holds their head and eyes in a theoretical resting position, it traces the actual optical path of light for thousands of real gaze directions simultaneously.
The system calculates across more than 3,000 gaze directions per lens. At each point, it models:
- The actual vertex distance from the back surface of the lens to the corneal apex
- The actual pantoscopic tilt of the frame on the patient’s face
- The actual wrap angle of the frame
- The near vision distance specific to the patient’s working habits
- The monocular pupillary distance for each eye independently
The result is a lens surface that is not designed for an average patient in an average frame. It is designed for this patient, in this frame, based on how she actually uses her vision.

The Clinical Significance of Point-by-Point Calculation
Optometrists familiar with wavefront aberrometry will recognize the underlying logic. Just as wavefront-guided LASIK corrects higher-order aberrations that standard ablation profiles ignore, IOT Digital Ray-Path 2 corrects the wearing-position aberrations that standard progressive designs accept as inevitable.
The clinical outcomes are measurable:
Wider usable visual fields. Because the lens surface is calculated to match the actual wearing geometry, optical performance across the corridor and periphery is closer to the design intent. Patients report a wider comfortable reading zone and more stable peripheral vision – particularly noticeable during head movement.
Faster adaptation. The aberrations that drive the most common adaptation complaints – swim, instability in peripheral motion, difficulty finding the corridor – are primarily geometry-related. When lens geometry matches the actual wearing position, the perceptual mismatch that triggers these complaints is reduced. Most patients with well-measured fitting parameters adapt within two to three days rather than two to three weeks.
More predictable outcomes in complex prescriptions. High add powers, high astigmatism, and strong sphere values all amplify the optical consequences of geometry mismatch. In these cases, the performance difference between a standard digital progressive and an IOT Digital Ray-Path lens is not marginal – it is the difference between a lens that works and one that generates a remake.
Why Fitting Measurements Matter More With This Technology
A lens calculated with IOT Digital Ray-Path 2 is only as accurate as the measurements fed into it.
This is worth stating explicitly because it changes how your team should approach the dispensing process. A standard progressive calculated on average parameters is relatively forgiving of minor measurement variations. A Digital Ray-Path lens is not – not because it is less precise, but because it uses those measurements directly. If the pantoscopic tilt you record is 8° and the frame actually sits at 12°, the calculation will optimize for a wearing geometry that doesn’t exist.
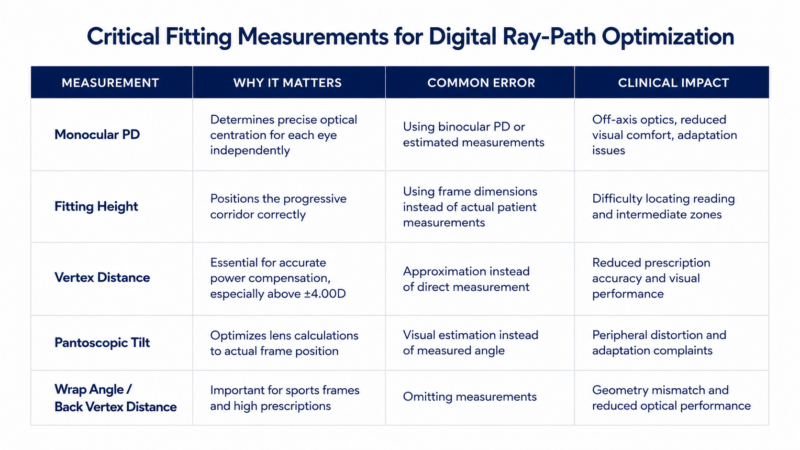
The measurements that must be accurate:
Monocular PD. Not binocular. Not estimated from pupillometer. Monocular PD measured at distance, with the frame the patient will be wearing. A 1mm error in centration shifts the optical center off-axis in a way that the Digital Ray-Path calculation cannot compensate for after the fact.
Fitting height. The vertical position of the fitting cross relative to the lower pupil margin, measured with the frame adjusted and the patient in natural head posture. Not the height you assume based on frame size — the height on this patient’s face, in this frame, after fitting.
Vertex distance. Particularly important in powers above ±4.00 diopters. An approximation is acceptable for standard designs. For Digital Ray-Path, an accurate measurement improves the calculation materially.
Pantoscopic tilt. The downward angle of the lens plane relative to vertical. Typically 8-12° for most frames. The instrument to measure this accurately is a protractor or a digital tiltmeter. Estimating by eye introduces enough variation to affect the calculation in sensitive patients.
Back vertex distance and wrap angle for high-power or sports applications.
Practices that invest in IOT Digital Ray-Path technology at the prescription level and then submit standard fitting parameters to the lab are not receiving the full benefit of the calculation system. The technology works as designed only when the parameters reflect the actual wearing geometry.
Where This Technology Lives in MIA LAB’s Lens Portfolio
MIA LAB’s Remedy progressive line is built on IOT Digital Ray-Path 2. The Remedy Plus, Remedy Max, and Remedy Camber designs all use this calculation engine as the foundation.
What differentiates the designs within the line is not the calculation platform – that’s consistent – but the corridor geometry and the adaptation strategy.
Remedy Plus uses a standard corridor approach with broader intermediate and distance zones. It performs well for most patients, particularly those transitioning from conventional progressives.
Remedy Max extends the near and intermediate zones, prioritizing reading area and screen use. For patients with significant occupational near demands, or patients who have struggled with narrow reading zones in previous progressives, this design addresses the core complaint directly.
Remedy Camber introduces Camber technology: a back-surface optimization that adjusts the curvature of the lens surface to the wearer’s natural line of sight, reducing the angular deviation between the optical axis and the gaze direction during habitual use. This results in cleaner peripheral vision and improved binocular balance, particularly in higher additions.
All three calculate the lens surface based on the wearing parameters your team submits – which means the quality of the clinical outcome is a direct function of the quality of the measurement process.
The Production Chain That Delivers the Calculation
The precision of IOT Digital Ray-Path 2 means nothing if the lab cannot execute the surface it specifies.
Digital freeform surfacing generates lens surfaces at micron-level tolerances. The calculation produces a data file specifying thousands of surface points — each precise to fractions of a micron. A generator that cannot hold that tolerance will produce a lens that diverges from the calculation in ways that appear at the periphery as blur or distortion.
At MIA LAB’s Hialeah facility, the surfacing equipment is calibrated to the tolerances required by Digital Ray-Path production. The lens is surfaced in-house. The coating is applied in-house. The quality check uses Focovision and Visionix lensmeters with ±1 micron accuracy. No step in that process is outsourced.
This matters for one specific reason: when you submit fitting parameters that represent the patient’s actual wearing geometry, the lens that arrives should match the calculation. Variability anywhere in the production chain – outsourced coating, off-calibration surfacing, lax QC – introduces errors that are invisible in the production record but visible to the patient.
For a closer look at how this production process works, the article on how prescription lenses are made describes each stage in detail.
The technology and the manufacturing have to match. One without the other is not digital freeform. It is digital freeform in name only.
How to Use This in the Dispensing Conversation
Most patients will not understand IOT Digital Ray-Path 2 by name. They don’t need to. What they understand is the outcome.
A practical script for the dispensing conversation:
“The lenses we’re making for you are calculated specifically for how you wear your frames – the angle they sit on your face, how far from your eyes, where you tend to look when you read. Most lenses are made with standard assumptions. These are made for you. That’s why patients typically adapt faster and find the viewing areas more comfortable.”
That explanation is accurate. It sets a realistic expectation. And it positions the premium as a clinical choice, not an upsell.
For patients who have previously failed with progressives, this framing is particularly important. Failure history is often geometry failure, not design failure. If their previous progressives were standard designs applied without precise fitting parameters, a Digital Ray-Path lens with accurate measurements is a materially different clinical offer – and deserves to be presented that way.
The Lab Decision Behind the Technology
Choosing to offer IOT Digital Ray-Path lenses is a technology decision. It is also a lab decision.
Not every independent optical lab that claims digital freeform capability is running Digital Ray-Path calculations or surfacing at the tolerances required to execute them accurately. The algorithm, the surfacing equipment, and the QC process have to be aligned. And the lab has to be willing to communicate directly when a prescription raises a production question.
Independent practices that have moved their Digital Ray-Path volume to MIA LAB typically report two changes: fewer adaptation complaints on their most complex cases, and fewer remake conversations on the patients who previously struggled with standard progressives. Both reduce staff time and increase patient confidence.
That is what a technology platform is supposed to do for a practice. Not change the name on the lens. Change the outcome for the patient.
FAQ: IOT Digital Ray-Path Lenses for Optometrists
- What is IOT Digital Ray-Path technology in progressive lenses?
IOT Digital Ray-Path is a computational lens design system developed by Indizen Optical Technologies. It traces light through the actual wearing geometry of the lens – accounting for vertex distance, pantoscopic tilt, wrap angle, and near vision distance – across more than 3,000 gaze directions. The result is a lens surface optimized for how a specific patient actually wears their glasses, rather than how an average patient wears an average frame.
- How does Digital Ray-Path differ from standard freeform surfacing?
Standard freeform surfacing generates a custom lens surface using conventional progressive design software. It is more precise than molded surfaces but still typically calculates using fixed wearing parameter assumptions. Digital Ray-Path 2 uses the actual fitting parameters measured for each patient to run a personalized ray trace calculation before surfacing begins. The surface geometry is different – specifically tailored to the measured wearing position.
- What measurements do I need for Digital Ray-Path lenses?
Accurate production requires monocular PD (not binocular), fitting height measured with the actual frame after adjustment, vertex distance, and pantoscopic tilt. Wrap angle is additional for wraparound or high-powered cases. These parameters should be measured precisely – not estimated. The calculation system uses them directly; any error in measurement produces a corresponding error in the lens.
- Do Digital Ray-Path lenses reduce remake rates?
In cases where remake was driven by geometry mismatch – the most common underlying cause of progressive adaptation failure – yes. Digital Ray-Path lenses address the root cause rather than the symptom. Practices that measure and submit accurate fitting parameters consistently report fewer adaptation complaints and lower remake frequency on complex prescriptions.
- Which patients benefit most from IOT Digital Ray-Path lenses?
High prescriptions (sphere above ±4.00 or cylinder above ±2.00), high add powers, patients with previously failed progressives, and patients with lifestyle-specific near vision demands benefit most. Patients in frequent frame-changing situations, where wearing geometry shifts between pairs, also benefit from the per-pair personalized calculation. For straightforward, low-power prescriptions with average fitting geometry, the performance difference compared to standard digital designs is smaller but still present.
- Is IOT Digital Ray-Path available in single vision lenses?
Yes. IOT’s calculation platform also supports single vision optimization, where the lens is calculated to minimize aberrations at the actual wearing position. This is particularly relevant in powers above ±3.00 diopters, where wearing position errors in conventional single vision lenses produce measurable distortion. MIA LAB’s Steady and Steady Plus single vision lenses apply this optimization.
- How do I explain Digital Ray-Path to patients who have failed with progressives before?
Frame the previous failure as a geometry problem, not a lens problem. Most patients who fail with progressives are wearing lenses calculated for average assumptions that don’t match their face or their habits. Digital Ray-Path lenses are calculated from their actual measurements. That’s a different clinical offer. Set realistic adaptation expectations – three to seven days for most patients with accurate measurements – and follow up at day three.
At MIA LAB, the Remedy progressive line is built on IOT Digital Ray-Path 2 technology, surfaced and finished in-house at our Hialeah facility. If you’re placing complex cases with a lab that isn’t executing Digital Ray-Path calculations and meeting micron-level surfacing tolerances, the technology isn’t reaching your patients. Learn more about opening a MIA LAB account.


